


 Sign Out
Sign Out
RISPERDAL/RISPERDAL CONSTA (risperidone) is not approved for the treatment of dementia‑related psychosis [see Warnings].
Risperdal: In two of four placebo-controlled trials in elderly patients with dementia-related psychosis, a higher incidence of mortality was observed in patients treated with furosemide plus RISPERDAL when compared to patients treated with RISPERDAL alone or with placebo plus furosemide. No pathological mechanism has been identified to explain this finding, and no consistent pattern for cause of death was observed.
Cerebrovascular Adverse Events, Including Stroke, in Elderly Patients with Dementia-Related Psychosis: Cerebrovascular adverse events (e.g., stroke, transient ischemic attack), including fatalities, were reported in patients (mean age 85 years; range 73-97) in trials of oral risperidone in elderly patients with dementia-related psychosis. In placebo‑controlled trials, there was a significantly higher incidence of cerebrovascular adverse events in patients treated with risperidone compared to patients treated with placebo. RISPERDAL/RISPERDAL CONSTA is not approved for the treatment of patients with dementia-related psychosis. [See Increased Mortality in Elderly Patients with Dementia-Related Psychosis as previously mentioned and Warnings.]
Neuroleptic Malignant Syndrome: Antipsychotic drugs can cause a potentially fatal symptom complex referred to as Neuroleptic Malignant Syndrome (NMS). Clinical manifestations of NMS include hyperpyrexia, muscle rigidity, altered mental status, and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia). Additional signs may include elevated creatine phosphokinase (CPK), myoglobinuria, rhabdomyolysis, and acute renal failure.
The diagnostic evaluation of patients with this syndrome is complicated. In arriving at a diagnosis, it is important to identify cases in which the clinical presentation includes both serious medical illness (e.g., pneumonia, systemic infection, etc.) and untreated or inadequately treated extrapyramidal signs and symptoms (EPS). Other important considerations in the differential diagnosis include central anticholinergic toxicity, heat stroke, drug fever, and primary central nervous system pathology.
The management of NMS should include: (1) immediate discontinuation of antipsychotic drugs and other drugs not essential to concurrent therapy; (2) intensive symptomatic treatment and medical monitoring; and (3) treatment of any concomitant serious medical problems for which specific treatments are available. There is no general agreement about specific pharmacological treatment regimens for uncomplicated NMS.
If a patient requires antipsychotic drug treatment after recovery from NMS, the potential reintroduction of drug therapy should be carefully considered. The patient should be carefully monitored, since recurrences of NMS have been reported.
Tardive Dyskinesia: A syndrome of potentially irreversible, involuntary, dyskinetic movements may develop in patients treated with antipsychotic drugs.
The risk of developing tardive dyskinesia and the likelihood that it will become irreversible are believed to increase as the duration of treatment and the total cumulative dose of antipsychotic drugs administered to the patient increase. However, the syndrome can develop, although much less commonly, after relatively brief treatment periods at low doses.
The syndrome may remit, partially or completely, if antipsychotic treatment is withdrawn. Antipsychotic treatment, itself, however, may suppress (or partially suppress) the signs and symptoms of the syndrome and thereby may possibly mask the underlying process. The effect that symptomatic suppression has upon the long-term course of the syndrome is unknown.
Given these considerations, RISPERDAL/RISPERDAL CONSTA should be prescribed in a manner that is most likely to minimize the occurrence of tardive dyskinesia. Chronic antipsychotic treatment should generally be reserved for patients who suffer from a chronic illness that: (1) is known to respond to antipsychotic drugs, and (2) for whom alternative, equally effective, but potentially less harmful treatments are not available or appropriate. In patients who do require chronic treatment, the smallest dose and the shortest duration of treatment producing a satisfactory clinical response should be sought. The need for continued treatment should be reassessed periodically.
If signs and symptoms of tardive dyskinesia appear in a patient treated with RISPERDAL/RISPERDAL CONSTA, drug discontinuation should be considered. However, some patients may require treatment with RISPERDAL/RISPERDAL CONSTA despite the presence of the syndrome.
Risperdal Consta: Although the prevalence of the syndrome appears to be highest among the elderly, especially elderly women, it is impossible to rely upon prevalence estimates to predict, at the inception of antipsychotic treatment, which patients are likely to develop the syndrome. Whether antipsychotic drug products differ in their potential to cause tardive dyskinesia is unknown.
Metabolic Changes: Atypical antipsychotic drugs have been associated with metabolic changes that may increase cardiovascular/cerebrovascular risk. These metabolic changes include hyperglycemia, dyslipidemia, and body weight gain. While all of the drugs in the class have been shown to produce some metabolic changes, each drug has its own specific risk profile.
Hyperglycemia and Diabetes Mellitus: Hyperglycemia and diabetes mellitus, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, have been reported in patients treated with atypical antipsychotics including RISPERDAL. Assessment of the relationship between atypical antipsychotic use and glucose abnormalities is complicated by the possibility of an increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population. Given these confounders, the relationship between atypical antipsychotic use and hyperglycemia-related adverse events is not completely understood. However, epidemiological studies suggest an increased risk of treatment-emergent hyperglycemia-related adverse events in patients treated with the atypical antipsychotics. Precise risk estimates for hyperglycemia-related adverse events in patients treated with atypical antipsychotics are not available.
Patients with an established diagnosis of diabetes mellitus who are started on atypical antipsychotics, including RISPERDAL, should be monitored regularly for worsening of glucose control. Patients with risk factors for diabetes mellitus (e.g., obesity, family history of diabetes) who are starting treatment with atypical antipsychotics, including RISPERDAL, should undergo fasting blood glucose testing at the beginning of treatment and periodically during treatment. Any patient treated with atypical antipsychotics, including RISPERDAL, should be monitored for symptoms of hyperglycemia including polydipsia, polyuria, polyphagia, and weakness. Patients who develop symptoms of hyperglycemia during treatment with atypical antipsychotics, including RISPERDAL, should undergo fasting blood glucose testing. In some cases, hyperglycemia has resolved when the atypical antipsychotic, including RISPERDAL, was discontinued; however, some patients required continuation of anti-diabetic treatment despite discontinuation of RISPERDAL.
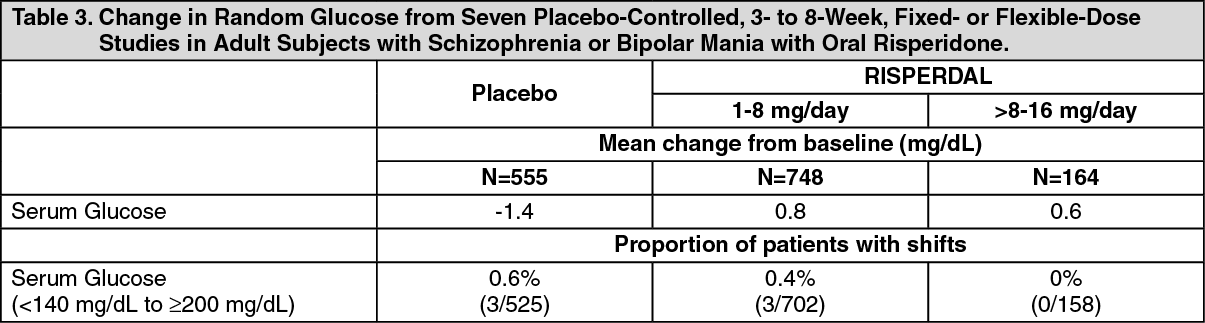
Pooled data from 3 double-blind, placebo-controlled studies in subjects with schizophrenia and 4 double-blind, placebo-controlled monotherapy studies in subjects with bipolar mania with oral risperidone are presented in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn longer-term, controlled and uncontrolled studies in adult subjects, RISPERDAL was associated with a mean change in glucose of +2.8 mg/dL at Week 24 (N=151) and +4.1 mg/dL at Week 48 (N=50).
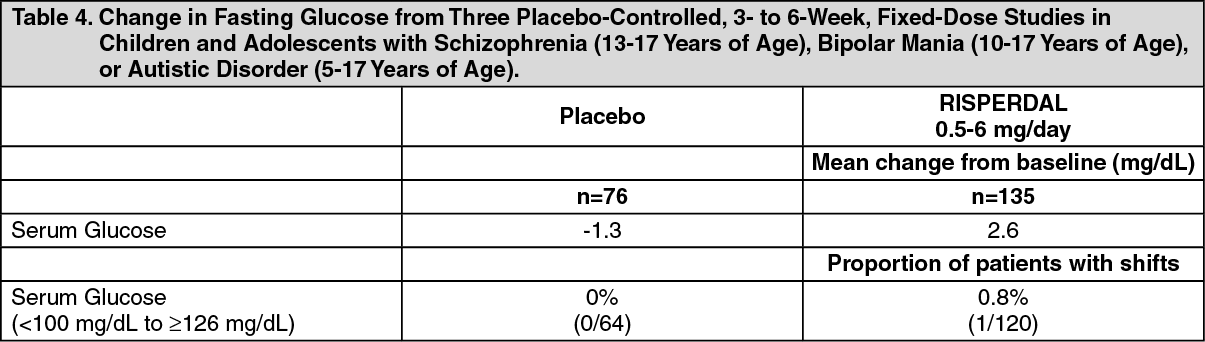
Risperdal: Data from the placebo-controlled 3- to 6-week study in children and adolescents with schizophrenia (13-17 years of age), bipolar mania (10-17 years of age), or autistic disorder (5-17 years of age) are presented in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn longer-term, uncontrolled, open-label extension pediatric studies, RISPERDAL was associated with a mean change in fasting glucose of +5.2 mg/dL at Week 24 (n=119).
Dyslipidemia: Undesirable alterations in lipids have been observed in patients treated with atypical antipsychotics.
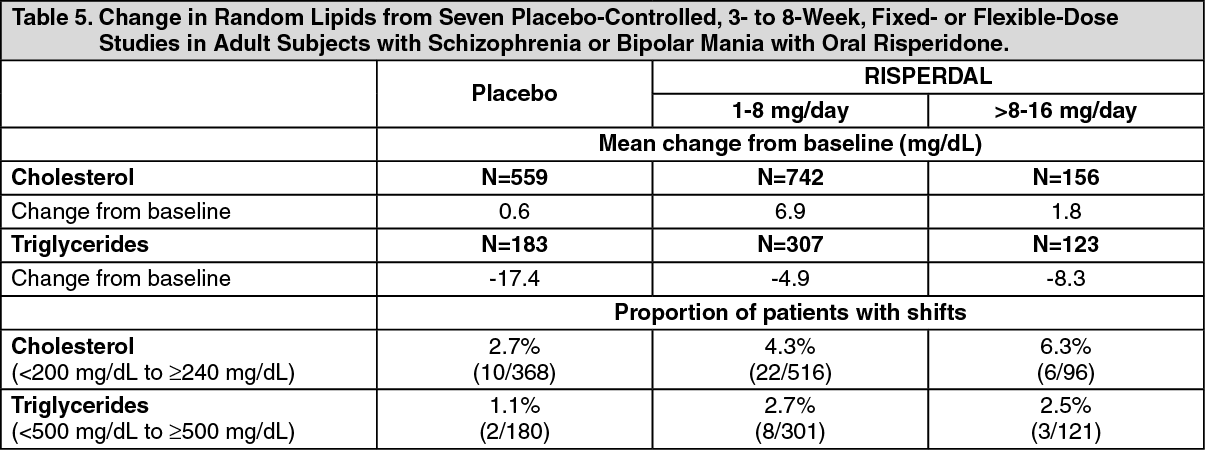
Pooled data from 7 placebo-controlled, 3- to 8-week, fixed- or flexible-dose studies in adult subjects with schizophrenia or bipolar mania are presented in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn longer-term, controlled and uncontrolled studies, RISPERDAL was associated with a mean change in (a) non-fasting cholesterol of +4.4 mg/dL at Week 24 (N=231) and +5.5 mg/dL at Week 48 (N=86); and (b) non-fasting triglycerides of +19.9 mg/dL at Week 24 (N=52).
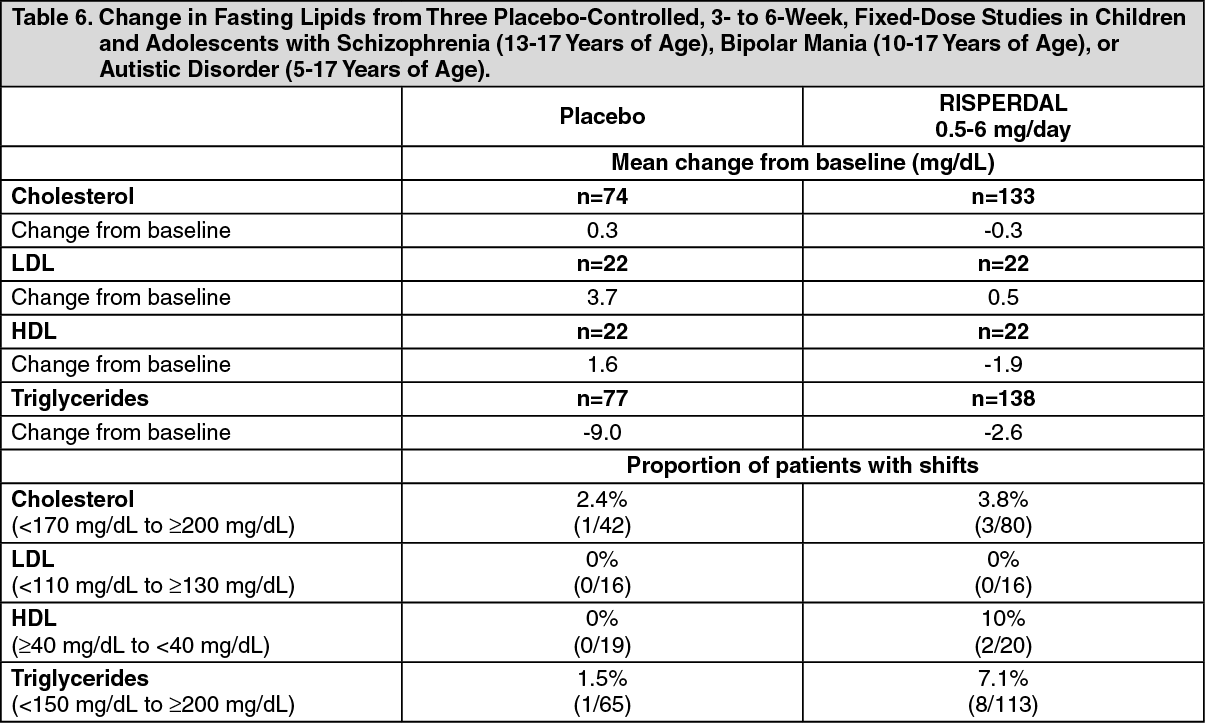
Risperdal: Pooled data from 3 placebo-controlled, 3- to 6-week, fixed-dose studies in children and adolescents with schizophrenia (13-17 years of age), bipolar mania (10-17 years of age), or autistic disorder (5-17 years of age) are presented in Table 6. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn longer-term, uncontrolled, open-label extension pediatric studies, RISPERDAL was associated with a mean change in (a) fasting cholesterol of +2.1 mg/dL at Week 24 (n=114); (b) fasting LDL of -0.2 mg/dL at Week 24 (n=103); (c) fasting HDL of +0.4 mg/dL at Week 24 (n=103); and (d) fasting triglycerides of +6.8 mg/dL at Week 24 (n=120).
Weight Gain: Weight gain has been observed with atypical antipsychotic use. Clinical monitoring of weight is recommended.
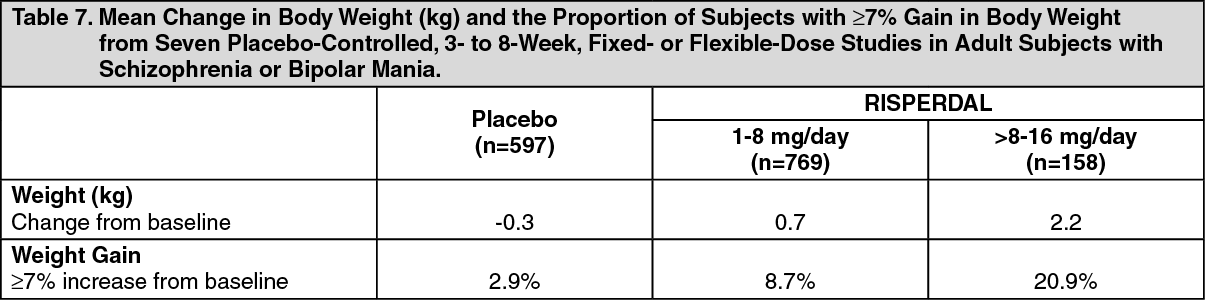
Risperdal: Data on mean changes in body weight and the proportion of subjects meeting a weight gain criterion of 7% or greater of body weight from 7 placebo-controlled, 3- to 8-week, fixed- or flexible-dose studies in adult subjects with schizophrenia or bipolar mania are presented in Table 7. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn longer-term, controlled and uncontrolled studies, RISPERDAL was associated with a mean change in weight of +4.3 kg at Week 24 (n=395) and +5.3 kg at Week 48 (n=203).
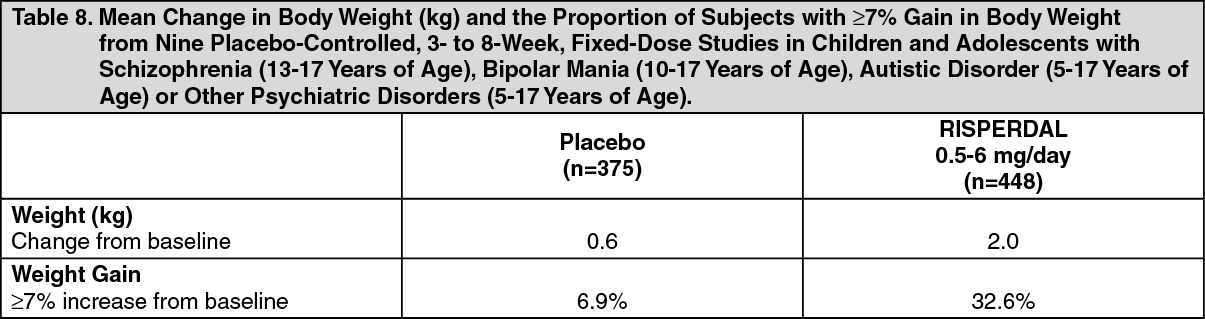
Data on mean changes in body weight and the proportion of subjects meeting the criterion of ≥7% gain in body weight from nine placebo-controlled, 3- to 8-week, fixed-dose studies in children and adolescents with schizophrenia (13-17 years of age), bipolar mania (10-17 years of age), autistic disorder (5-17 years of age), or other psychiatric disorders (5-17 years of age) are presented in Table 8. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn longer-term, uncontrolled, open-label extension pediatric studies, RISPERDAL was associated with a mean change in weight of +5.5 kg at Week 24 (n=748) and +8.0 kg at Week 48 (n=242).
In a long-term, open-label extension study in adolescent patients with schizophrenia, weight increase was reported as a treatment-emergent adverse event in 14% of patients. In 103 adolescent patients with schizophrenia, a mean increase of 9.0 kg was observed after 8 months of RISPERDAL treatment. The majority of that increase was observed within the first 6 months. The average percentiles at baseline and 8 months, respectively, were 56 and 72 for weight, 55 and 58 for height, and 51 and 71 for body mass index.
In long-term, open-label trials (studies in patients with autistic disorder or other psychiatric disorders), a mean increase of 7.5 kg after 12 months of RISPERDAL treatment was observed, which was higher than the expected normal weight gain (approximately 3 to 3.5 kg per year adjusted for age, based on Centers for Disease Control and Prevention normative data). The majority of that increase occurred within the first 6 months of exposure to RISPERDAL. The average percentiles at baseline and 12 months, respectively, were 49 and 60 for weight, 48 and 53 for height, and 50 and 62 for body mass index.
In one 3-week, placebo-controlled trial in children and adolescent patients with acute manic or mixed episodes of bipolar I disorder, increases in body weight were higher in the RISPERDAL groups than the placebo group, but not dose related (1.90 kg in the RISPERDAL 0.5‑2.5 mg group, 1.44 kg in the RISPERDAL 3‑6 mg group, and 0.65 kg in the placebo group). A similar trend was observed in the mean change from baseline in body mass index.
When treating pediatric patients with RISPERDAL for any indication, weight gain should be assessed against that expected with normal growth.
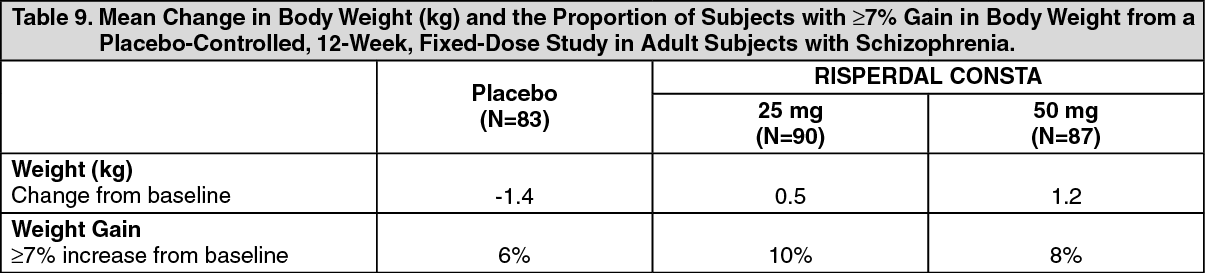
Risperdal Consta: Data from a placebo-controlled, 12-week, fixed-dose study in adult subjects with schizophrenia are presented in Table 9. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn an uncontrolled, longer-term, open-label study, RISPERDAL CONSTA was associated with a mean change in weight of +2.1 kg at Week 24 (N=268) and +2.8 kg at Week 50 (N=199).
Hyperprolactinemia: As with other drugs that antagonize dopamine D2 receptors, risperidone elevates prolactin levels and the elevation persists during chronic administration. Risperidone is associated with higher levels of prolactin elevation than other antipsychotic agents.
Hyperprolactinemia may suppress hypothalamic GnRH, resulting in reduced pituitary gonadotropin secretion. This, in turn, may inhibit reproductive function by impairing gonadal steroidogenesis in both female and male patients. Galactorrhea, amenorrhea, gynecomastia, and impotence have been reported in patients receiving prolactin-elevating compounds. Long-standing hyperprolactinemia when associated with hypogonadism may lead to decreased bone density in both female and male subjects.
Tissue culture experiments indicate that approximately one-third of human breast cancers are prolactin dependent in vitro, a factor of potential importance if the prescription of these drugs is contemplated in a patient with previously detected breast cancer. An increase in pituitary gland, mammary gland, and pancreatic islet cell neoplasia (mammary adenocarcinomas, pituitary and pancreatic adenomas) was observed in the risperidone carcinogenicity studies conducted in mice and rats [see Pharmacology: Toxicology: Nonclinical Toxicology under Actions]. Neither clinical studies nor epidemiologic studies conducted to date have shown an association between chronic administration of this class of drugs and tumorigenesis in humans; the available evidence is considered too limited to be conclusive at this time.
Orthostatic Hypotension: RISPERDAL/RISPERDAL CONSTA may induce orthostatic hypotension associated with dizziness, tachycardia, and in some patients, syncope, especially during the initial dose-titration period with oral risperidone, probably reflecting its alpha-adrenergic antagonistic properties.
Monitoring of orthostatic vital signs should be considered in patients for whom this is of concern. A dose reduction should be considered if hypotension occurs.
Clinically significant hypotension has been observed with concomitant use of oral RISPERDAL and antihypertensive medication.
Risperdal: Syncope was reported in 0.2% (6/2607) of RISPERDAL-treated patients in Phase 2 and 3 studies in adults with schizophrenia. The risk of orthostatic hypotension and syncope may be minimized by limiting the initial dose to 2 mg total (either once daily or 1 mg twice daily) in normal adults and 0.5 mg twice daily in the elderly and patients with renal or hepatic impairment [see Dosage & Administration].
RISPERDAL should be used with particular caution in patients with known cardiovascular disease (history of myocardial infarction or ischemia, heart failure, or conduction abnormalities), cerebrovascular disease, and conditions which would predispose patients to hypotension, e.g., dehydration and hypovolemia.
Risperdal Consta: Syncope was reported in 0.8% (12/1499 patients) of patients treated with RISPERDAL CONSTA in multiple-dose studies. Patients should be instructed in nonpharmacologic interventions that help to reduce the occurrence of orthostatic hypotension (e.g., sitting on the edge of the bed for several minutes before attempting to stand in the morning and slowly rising from a seated position).
RISPERDAL CONSTA should be used with particular caution in (1) patients with known cardiovascular disease (history of myocardial infarction or ischemia, heart failure, or conduction abnormalities), cerebrovascular disease, and conditions which would predispose patients to hypotension, e.g., dehydration and hypovolemia, and (2) in the elderly and patients with renal or hepatic impairment.
Falls: Somnolence, postural hypotension, motor and sensory instability have been reported with the use of antipsychotics, including RISPERDAL/RISPERDAL CONSTA, which may lead to falls and, consequently, fractures or other fall-related injuries. For patients, particularly the elderly, with diseases, conditions, or medications that could exacerbate these effects, assess the risk of falls when initiating antipsychotic treatment and recurrently for patients on long-term antipsychotic therapy.
Leukopenia, Neutropenia, and Agranulocytosis: Class Effect: In clinical trial and/or postmarketing experience, events of leukopenia/neutropenia have been reported temporally related to antipsychotic agents, including RISPERDAL/RISPERDAL CONSTA. Agranulocytosis has also been reported.
Possible risk factors for leukopenia/neutropenia include pre-existing low white blood cell count (WBC) and history of drug-induced leukopenia/neutropenia. Patients with a history of a clinically significant low WBC or a drug-induced leukopenia/neutropenia should have their complete blood count (CBC) monitored frequently during the first few months of therapy and discontinuation of RISPERDAL/RISPERDAL CONSTA should be considered at the first sign of a clinically significant decline in WBC in the absence of other causative factors.
Patients with clinically significant neutropenia should be carefully monitored for fever or other symptoms or signs of infection and treated promptly if such symptoms or signs occur. Patients with severe neutropenia (absolute neutrophil count <1000/mm3) should discontinue RISPERDAL/RISPERDAL CONSTA and have their WBC followed until recovery.
Potential for Cognitive and Motor Impairment: Since risperidone has the potential to impair judgment, thinking, or motor skills, patients should be cautioned about operating hazardous machinery, including automobiles, until they are reasonably certain that treatment with RISPERDAL/RISPERDAL CONSTA does not affect them adversely.
Risperdal: Somnolence was a commonly reported adverse reaction associated with RISPERDAL treatment, especially when ascertained by direct questioning of patients. This adverse reaction is dose-related, and in a study utilizing a checklist to detect adverse events, 41% of the high-dose patients (RISPERDAL 16 mg/day) reported somnolence compared to 16% of placebo patients. Direct questioning is more sensitive for detecting adverse events than spontaneous reporting, by which 8% of RISPERDAL 16 mg/day patients and 1% of placebo patients reported somnolence as an adverse reaction.
Risperdal Consta: Somnolence was reported by 5% of patients treated with RISPERDAL CONSTA in multiple‑dose trials.
Seizures: RISPERDAL/RISPERDAL CONSTA should be used cautiously in patients with a history of seizures.
Risperdal: During premarketing testing in adult patients with schizophrenia, seizures occurred in 0.3% (9/2607) of RISPERDAL‑treated patients, two in association with hyponatremia.
Risperdal Consta: During premarketing testing, seizures occurred in 0.3% (5/1499 patients) of patients treated with RISPERDAL CONSTA.
Dysphagia: Esophageal dysmotility and aspiration have been associated with antipsychotic drug use. Aspiration pneumonia is a common cause of morbidity and mortality in patients with advanced Alzheimer's dementia. RISPERDAL/RISPERDAL CONSTA and other antipsychotic drugs should be used cautiously in patients at risk for aspiration pneumonia. [See Increased Mortality in Elderly Patients with Dementia-Related Psychosis as previously mentioned and Warnings.]
Priapism: Priapism has been reported during postmarketing surveillance [see Adverse Reactions]. Severe priapism may require surgical intervention.
Thrombotic Thrombocytopenic Purpura (TTP): Risperdal Consta: A single case of TTP was reported in a 28 year-old female patient receiving oral RISPERDAL in a large, open premarketing experience (approximately 1300 patients). She experienced jaundice, fever, and bruising, but eventually recovered after receiving plasmapheresis. The relationship to RISPERDAL therapy is unknown.
Body Temperature Regulation: Disruption of body temperature regulation has been attributed to antipsychotic agents. Both hyperthermia and hypothermia have been reported in association with RISPERDAL/RISPERDAL CONSTA use. Caution is advised when prescribing for patients who will be exposed to temperature extremes.
Administration: Risperdal Consta: RISPERDAL CONSTA should be injected into the deltoid or gluteal muscle, and care must be taken to avoid inadvertent injection into a blood vessel. [See Dosage & Administration and Adverse Reactions.]
Antiemetic Effect: Risperdal Consta: Risperidone has an antiemetic effect in animals; this effect may also occur in humans, and may mask signs and symptoms of overdosage with certain drugs or of conditions such as intestinal obstruction, Reye's syndrome, and brain tumor.
Use in Patients with Concomitant Illness: Risperdal Consta: Clinical experience with RISPERDAL CONSTA in patients with certain concomitant systemic illnesses is limited. Patients with Parkinson's Disease or Dementia with Lewy Bodies who receive antipsychotics, including RISPERDAL CONSTA, are reported to have an increased sensitivity to antipsychotic medications. Manifestations of this increased sensitivity have been reported to include confusion, obtundation, postural instability with frequent falls, extrapyramidal symptoms, and clinical features consistent with the neuroleptic malignant syndrome.
Caution is advisable when using RISPERDAL CONSTA in patients with diseases or conditions that could affect metabolism or hemodynamic responses. RISPERDAL CONSTA has not been evaluated or used to any appreciable extent in patients with a recent history of myocardial infarction or unstable heart disease. Patients with these diagnoses were excluded from clinical studies during the product's premarket testing.
Increased plasma concentrations of risperidone and 9-hydroxyrisperidone occur in patients with severe renal impairment (creatinine clearance <30 mL/min/1.73 m2) treated with oral RISPERDAL; an increase in the free fraction of risperidone is also seen in patients with severe hepatic impairment. Patients with renal or hepatic impairment should be carefully titrated on oral RISPERDAL before treatment with RISPERDAL CONSTA is initiated at a dose of 25 mg. A lower initial dose of 12.5 mg may be appropriate when clinical factors warrant dose adjustment, such as in patients with renal or hepatic impairment [see Dosage & Administration].
Osteodystrophy and Tumors in Animals: Risperdal Consta: RISPERDAL CONSTA produced osteodystrophy in male and female rats in a 1-year toxicity study and a 2-year carcinogenicity study at a dose of 40 mg/kg administered IM every 2 weeks.
RISPERDAL CONSTA produced renal tubular tumors (adenoma, adenocarcinoma) and adrenomedullary pheochromocytomas in male rats in the 2-year carcinogenicity study at 40 mg/kg administered IM every 2 weeks. In addition, RISPERDAL CONSTA produced an increase in a marker of cellular proliferation in renal tissue in males in the 1-year toxicity study and in renal tumor-bearing males in the 2-year carcinogenicity study at 40 mg/kg administered IM every 2 weeks. (Cellular proliferation was not measured at the low dose or in females in either study.)
The effect dose for osteodystrophy and the tumor findings is 8 times the IM maximum recommended human dose (MRHD) (50 mg) on a mg/m2 basis and is associated with a plasma exposure (AUC) 2 times the expected plasma exposure (AUC) at the IM MRHD. The no-effect dose for these findings was 5 mg/kg (equal to the IM MRHD on a mg/m2 basis). Plasma exposure (AUC) at the no-effect dose was one third the expected plasma exposure (AUC) at the IM MRHD.
Neither the renal or adrenal tumors, nor osteodystrophy, were seen in studies of orally administered risperidone. Osteodystrophy was not observed in dogs at doses up to 14 times (based on AUC) the IM MRHD in a 1-year toxicity study.
The renal tubular and adrenomedullary tumors in male rats and other tumor findings are described in more detail in Pharmacology: Toxicology: Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility under Actions.
The relevance of these findings to human risk is unknown.
Intraoperative Floppy Iris Syndrome: Intraoperative Floppy Iris Syndrome (IFIS) has been observed during cataract surgery in patients treated with medicines with alpha1a-adrenergic antagonist effect, including RISPERDAL/RISPERDAL CONSTA [see Adverse Reactions].
IFIS may increase the risk of eye complications during and after the operation. Current or past use of medicines with alpha1a-adrenergic antagonist effect should be made known to the ophthalmic surgeon in advance of surgery. The potential benefit of stopping alpha1 blocking therapy prior to cataract surgery has not been established and must be weighed against the risk of stopping the antipsychotic therapy.
Drug Abuse and Dependence: Controlled Substance: RISPERDAL/RISPERDAL CONSTA (risperidone) is not a controlled substance.
Abuse: RISPERDAL/RISPERDAL CONSTA has not been systematically studied in animals or humans for its potential for abuse.
Risperdal: While the clinical trials did not reveal any tendency for any drug-seeking behavior, these observations were not systematic and it is not possible to predict on the basis of this limited experience the extent to which a CNS-active drug will be misused, diverted, and/or abused once marketed. Consequently, patients should be evaluated carefully for a history of drug abuse, and such patients should be observed closely for signs of RISPERDAL misuse or abuse (e.g., development of tolerance, increases in dose, drug-seeking behavior).
Risperdal Consta: Because RISPERDAL CONSTA is to be administered by health care professionals, the potential for misuse or abuse by patients is low.
Dependence: RISPERDAL/RISPERDAL CONSTA has not been systematically studied in animals or humans for its potential for tolerance or physical dependence.
Renal Impairment: Risperdal: In patients with moderate to severe (Clcr 59 to 15 mL/min) renal disease, clearance of the sum of risperidone and its active metabolite decreased by 60%, compared to young healthy subjects. RISPERDAL doses should be reduced in patients with renal disease [see Dosage & Administration].
Hepatic Impairment: Risperdal: While the pharmacokinetics of risperidone in subjects with liver disease were comparable to those in young healthy subjects, the mean free fraction of risperidone in plasma was increased by about 35% because of the diminished concentration of both albumin and α1-acid glycoprotein. RISPERDAL doses should be reduced in patients with liver disease [see Dosage & Administration].
Patients with Parkinson's Disease or Lewy Body Dementia: Risperdal: Patients with Parkinson's Disease or Dementia with Lewy Bodies can experience increased sensitivity to RISPERDAL. Manifestations can include confusion, obtundation, postural instability with frequent falls, extrapyramidal symptoms, and clinical features consistent with neuroleptic malignant syndrome.
Use in Children: Juvenile Animal Studies: Juvenile dogs were treated with oral risperidone from weeks 10 to 50 of age (equivalent to the period of childhood through adolescence in humans), at doses of 0.31, 1.25, or 5 mg/kg/day, which are 1.2, 3.4, and 13.5 times the MRHD of 6 mg/day for children, based on mg/m2 body surface area. Bone length and density were decreased with a no-effect dose of 0.31 mg/kg/day; this dose produced plasma AUC of risperidone plus its active metabolite paliperidone (9-hydroxy-risperidone) that were similar to those in children and adolescents receiving the MRHD of 6 mg/day. In addition, sexual maturation was delayed at all doses in both males and females. The previously mentioned effects showed little or no reversibility in females after a 12 week drug-free recovery period.
Juvenile rats, treated with oral risperidone from days 12 to 50 of age (equivalent to the period of infancy through adolescence in humans) showed impaired learning and memory performance (reversible only in females), with a no-effect dose of 0.63 mg/kg/day which is 0.5 times the MRHD of 6 mg/day for children, based on mg/m2 body surface area. This dose produced plasma AUC of risperidone plus paliperidone about half the exposure observed in humans at the MRHD. No other consistent effects on neurobehavioral or reproductive development were seen up to the highest tested dose of 1.25 mg/kg/day which is 1 time the MRHD and produced plasma AUC of risperidone plus paliperidone that were about two thirds of those observed in humans at the MRHD of 6 mg/day for children.
Risperdal: Approved Pediatric Indications: Schizophrenia: The efficacy and safety of RISPERDAL in the treatment of schizophrenia were demonstrated in 417 adolescents, aged 13 - 17 years, in two short-term (6 and 8 weeks, respectively) double-blind controlled trials [see Indications/Uses, Adverse Reactions, and Pharmacology: Pharmacodynamics: Clinical Studies under Actions]. Additional safety and efficacy information was also assessed in one long-term (6-month) open-label extension study in 284 of these adolescent patients with schizophrenia.
Safety and effectiveness of RISPERDAL in children less than 13 years of age with schizophrenia have not been established.
Bipolar I Disorder: The efficacy and safety of RISPERDAL in the short-term treatment of acute manic or mixed episodes associated with Bipolar I Disorder in 169 children and adolescent patients, aged 10 - 17 years, were demonstrated in one double-blind, placebo-controlled, 3-week trial [see Indications/Uses, Adverse Reactions, and Pharmacology: Pharmacodynamics: Clinical Studies under Actions].
Safety and effectiveness of RISPERDAL in children less than 10 years of age with bipolar disorder have not been established.
Autistic Disorder: The efficacy and safety of RISPERDAL in the treatment of irritability associated with autistic disorder were established in two 8-week, double-blind, placebo-controlled trials in 156 children and adolescent patients, aged 5 to 16 years [see Indications/Uses, Adverse Reactions, and Pharmacology: Pharmacodynamics: Clinical Studies under Actions]. Additional safety information was also assessed in a long-term study in patients with autistic disorder, or in short- and long-term studies in more than 1200 pediatric patients with psychiatric disorders other than autistic disorder, schizophrenia, or bipolar mania who were of similar age and weight, and who received similar dosages of RISPERDAL as patients treated for irritability associated with autistic disorder.
A third study was a 6-week, multicenter, randomized, double-blind, placebo-controlled, fixed-dose study to evaluate the efficacy and safety of a lower than recommended dose of risperidone in subjects 5 to 17 years of age with autistic disorder and associated irritability, and related behavioral symptoms. There were two weight-based, fixed doses of risperidone (high-dose and low-dose). The high dose was 1.25 mg per day for patients weighing 20 to < 45 kg, and it was 1.75 mg per day for patients weighing > 45 kg. The low dose was 0.125 mg per day for patients for patients weighing 20 to < 45 kg, and it was 0.175 mg per day for patients weighing > 45 kg. The study demonstrated the efficacy of high-dose risperidone, but it did not demonstrate efficacy for low-dose risperidone.
Adverse Reactions in Pediatric Patients: Tardive Dyskinesia: In clinical trials in 1885 children and adolescents treated with RISPERDAL, 2 (0.1%) patients were reported to have tardive dyskinesia, which resolved on discontinuation of RISPERDAL treatment [see also Tardive Dyskinesia as previously mentioned].
Weight Gain: Weight gain has been observed in children and adolescents during treatment with RISPERDAL. Clinical monitoring of weight is recommended during treatment.
Data derive from short-term placebo-controlled trials and longer-term uncontrolled studies in pediatric patients (ages 5 to 17 years) with schizophrenia, bipolar disorder, autistic disorder, or other psychiatric disorders. In the short-term trials (3 to 8 weeks), the mean weight gain for RISPERDAL-treated patients was 2 kg, compared to 0.6 kg for placebo-treated patients. In these trials, approximately 33% of the RISPERDAL group had weight gain >7%, compared to 7% in the placebo group. In longer-term, uncontrolled, open-label pediatric studies, the mean weight gain was 5.5 kg at Week 24 and 8 kg at Week 48 [see Metabolic Changes as previously mentioned and Adverse Reactions].
Somnolence: Somnolence was frequently observed in placebo-controlled clinical trials of pediatric patients with autistic disorder. Most cases were mild or moderate in severity. These events were most often of early onset with peak incidence occurring during the first two weeks of treatment, and transient with a median duration of 16 days. Somnolence was the most commonly observed adverse reaction in the clinical trial of bipolar disorder in children and adolescents, as well as in the schizophrenia trials in adolescents. As was seen in the autistic disorder trials, these adverse reactions were most often of early onset and transient in duration [see Adverse Reactions]. Patients experiencing persistent somnolence may benefit from a change in dosing regimen [see Dosage & Administration].
Hyperprolactinemia: RISPERDAL has been shown to elevate prolactin levels in children and adolescents as well as in adults [see Hyperprolactinemia as previously mentioned]. In double-blind, placebo-controlled studies of up to 8 weeks duration in children and adolescents (aged 5 to 17 years) with autistic disorder or psychiatric disorders other than autistic disorder, schizophrenia, or bipolar mania, 49% of patients who received RISPERDAL had elevated prolactin levels compared to 2% of patients who received placebo. Similarly, in placebo-controlled trials in children and adolescents (aged 10 to 17 years) with bipolar disorder, or adolescents (aged 13 to 17 years) with schizophrenia, 82-87% of patients who received RISPERDAL had elevated levels of prolactin compared to 3‑7% of patients on placebo. Increases were dose-dependent and generally greater in females than in males across indications.
In clinical trials in 1885 children and adolescents, galactorrhea was reported in 0.8% of RISPERDAL-treated patients and gynecomastia was reported in 2.3% of RISPERDAL-treated patients.
Growth and Sexual Maturation: The long-term effects of RISPERDAL on growth and sexual maturation have not been fully evaluated in children and adolescents.
Risperdal Consta: Safety and effectiveness of RISPERDAL CONSTA in pediatric patients have not been established. However, juvenile animal toxicology studies have been conducted with oral risperidone.
Use in the Elderly: Risperdal: Clinical studies of RISPERDAL in the treatment of schizophrenia did not include sufficient numbers of patients aged 65 and over to determine whether or not they respond differently than younger patients. Other reported clinical experience has not identified differences in responses between elderly and younger patients. In general, a lower starting dose is recommended for an elderly patient, reflecting a decreased pharmacokinetic clearance in the elderly, as well as a greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy [see Pharmacology: Pharmacokinetics under Actions and Dosage & Administration]. While elderly patients exhibit a greater tendency to orthostatic hypotension, its risk in the elderly may be minimized by limiting the initial dose to 0.5 mg twice daily followed by careful titration [see Orthostatic Hypotension as previously mentioned]. Monitoring of orthostatic vital signs should be considered in patients for whom this is of concern.
This drug is substantially excreted by the kidneys, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function [see Dosage & Administration].
Risperdal Consta: In an open-label study, 57 clinically stable, elderly patients (≥ 65 years old) with schizophrenia or schizoaffective disorder received RISPERDAL CONSTA every 2 weeks for up to 12 months. In general, no differences in the tolerability of RISPERDAL CONSTA were observed between otherwise healthy elderly and nonelderly patients. Therefore, dosing recommendations for otherwise healthy elderly patients are the same as for nonelderly patients. Because elderly patients exhibit a greater tendency to orthostatic hypotension than nonelderly patients, elderly patients should be instructed in nonpharmacologic interventions that help to reduce the occurrence of orthostatic hypotension (e.g., sitting on the edge of the bed for several minutes before attempting to stand in the morning and slowly rising from a seated position). In addition, monitoring of orthostatic vital signs should be considered in elderly patients for whom orthostatic hypotension is of concern [see Orthostatic Hypotension as previously mentioned].
Concomitant use with Furosemide in Elderly Patients with Dementia-Related Psychosis: In two of four placebo-controlled trials in elderly patients with dementia-related psychosis, a higher incidence of mortality was observed in patients treated with furosemide plus oral risperidone when compared to patients treated with oral risperidone alone or with oral placebo plus furosemide. No pathological mechanism has been identified to explain this finding, and no consistent pattern for cause of death was observed. An increase of mortality in elderly patients with dementia-related psychosis was seen with the use of oral risperidone regardless of concomitant use with furosemide. RISPERDAL CONSTA is not approved for the treatment of patients with dementia-related psychosis. [See Increased Mortality in Elderly Patients with Dementia-Related Psychosis as previously mentioned and Warnings.]